Documentation is repeatedly cited among the biggest time burdens in speech-language pathology, and burnout is widely reported as high — especially in school-based caseloads. The note that’s supposed to capture five minutes of clinical reasoning too often becomes the thing you finish in the parking lot.
This article is a section-by-section guide to writing a defensible articulation SOAP note — Subjective, Objective, Assessment, and Plan — with copy-ready worked examples across the articulation hierarchy and a reusable cue-level table you can paste from. It also covers the two questions vendor blogs skip: whether SOAP is even required, and how SOAP relates to the faster DAP format.
Here’s the thesis up front, because it changes how you read everything below: a SOAP note should be a byproduct of good practice, not a separate after-hours chore. The hard part of an articulation note isn’t formatting four sections — it’s having an accurate accuracy percentage, the right cue level, and the target sound and position captured during the session. Get the data collection right and the note nearly writes itself.
One disclaimer before the templates, in the same spirit as our IEP goals guide: every example here is a template, not a substitute for your clinical judgment or your district’s and payers’ documentation conventions. Use student initials rather than full names in any sample note you adapt, and adjust the criteria to the student in front of you.
What Is a SOAP Note? (Subjective, Objective, Assessment, Plan)
SOAP stands for Subjective, Objective, Assessment, Plan. Each section has a defined job:
- Subjective — what the client or caregiver reports, plus observed engagement and affect.
- Objective — the measurable session data (target sound, position, hierarchy level, accuracy, cue level).
- Assessment — your clinical interpretation of that data.
- Plan — what happens next session and at home.
The format isn’t a speech-pathology invention. The SOAP note comes from Dr. Lawrence Weed’s problem-oriented medical record, first published in the mid-1960s (1964, then popularized through a 1968 New England Journal of Medicine article). Weed designed it to organize complex patients with multiple problems systematically — which is exactly why the Subjective/Objective split still earns its keep in team and payer contexts decades later. Separating what was reported from what was measured is the whole point.
For speech-language pathologists, “what does SOAP stand for” and “what goes in each section” have the same answer in every setting: the four sections above, applied to a therapy session instead of a hospital admission. The through-line that organizes the rest of this article is that each section answers exactly one question:
- S: How did the session feel, and what was reported?
- O: What are the numbers?
- A: What do the numbers mean?
- P: What happens next?
Keep that mapping in mind and the most common documentation mistakes — covered later — become obvious. Here’s the whole structure as a single bookmarkable table, with an articulation example fragment for each section:
| Section | Question it answers | Articulation example fragment |
|---|---|---|
| Subjective | How did the session feel? What was reported? | ”Caregiver reports T.M. practiced /r/ word cards twice this week; student engaged and on-task throughout (engagement: Good).” |
| Objective | What are the numbers? | ”T.M. produced /r/ in the initial position of single words with 80% accuracy (16/20) given moderate cues.” |
| Assessment | What do the numbers mean? | ”Accuracy improved 20 points over baseline (60%), indicating readiness to fade to minimal cues.” |
| Plan | What happens next? | ”Advance to phrase level next session; reduce to minimal cues; assign 10 initial-/r/ words for home practice.” |
The rest of this guide walks each one in clinical detail.
The Subjective Section: Engagement and Report
The Subjective section captures everything that isn’t a measured number: the caregiver or teacher report, the student’s own self-report, observed engagement and affect, and relevant context — illness, a missed week of home practice, a rough morning in the classroom. It’s the section that explains the Objective numbers when they wobble.
For a school-age articulation caseload, the most reliable thing to anchor here is engagement. Sound Safari captures it on a four-level scale — Excellent / Good / Fair / Poor — so the Subjective section is never left blank or filled with a vague “did fine.” A consistent engagement scale also makes the section comparable across sessions: “engagement dropped from Good to Fair, coinciding with reported illness” is a real clinical observation.
There’s one clean rule that keeps the whole note defensible: don’t put measurable data in Subjective, and don’t put subjective impressions in Objective. Accuracy percentages, trial counts, and cue levels belong in the Objective section. Engagement, affect, and what the family told you belong here. And vague “did well” language belongs in neither — it’s not a measurement and it’s not a useful report.
Compare these two Subjective lines:
Weak: “Student did well today and seemed happy.”
Strong: “Caregiver reports S.R. completed home practice 4 of 5 assigned days. Student arrived on-task and engaged throughout the session (engagement: Good); no behavioral or attentional concerns noted.”
For most school-based articulation work, Subjective is the lightest of the four sections — far lighter than in a medical or mental-health SOAP note, where the client’s subjective report carries diagnostic weight. But it still earns its place: it documents the state and the report that explain why the Objective numbers came out the way they did. When accuracy drops, the Subjective section is often where the reason already lives.
The Objective Section: The Data That Makes a Note Defensible
This is the heart of the note, and the section payers, IEP teams, and your future self actually read. A defensible articulation Objective section reports five measurable elements, and this is a cross-source standard, not one vendor’s house style — TheraPlatform and SimplePractice both teach the same spine:
- Target sound (e.g., /r/)
- Word position (initial, medial, final)
- Level of the articulation hierarchy (isolation, syllable, word, phrase, sentence, conversation)
- Accuracy percentage — always as a fraction, correct over total (e.g., 16/20 = 80%)
- Cue / prompting level
Sound Safari’s session data maps directly onto this spine. Scoring uses Correct / Incorrect — plus an optional third Approximate score for emerging productions — and the correct count over total trials produces the accuracy fraction. The session is reported at one of four prompting levels, which is the cue dimension:
| Prompting level | What the student gets | Maps to |
|---|---|---|
| Maximum | Picture + Word + Model | Maximal cueing |
| Moderate | Picture + Word | Moderate cueing |
| Minimal | Word only | Minimal cueing |
| Independent | Picture only / no prompts | Independent |
Here is the authoritative copy-ready pattern, drawn straight from TheraPlatform’s articulation example:
Defensible: “Client produced /r/ in the initial position of single words with 80% accuracy given moderate cues.”
Now the version that gets a note flagged in an audit:
Poor: “Worked on /r/ words today. Client did a good job and is making progress.”
The second one has no sound position, no level, no accuracy, and no cue level — nothing another clinician could act on. It’s the single most common Objective failure.
When accuracy varies by cue level, report each band. SimplePractice’s worked /k/ example shows the convention cleanly: word-initial /k/ at 70% (14/20) of opportunities given a gestural cue, 30% (6/20) without any cue, then 80% (8/10) after a model. That breakdown is far more useful than a single blended number, because it shows exactly where the student is along the fading continuum.
Notice what all of this requires: an accurate accuracy percentage, the right cue level, and the target sound and position — captured while the session is running, not reconstructed from memory afterward. That collection step is the genuinely hard part of documentation, and it’s the part every documentation tool quietly assumes you’ve already solved. Sound Safari is built to capture it during practice: the three-point scoring, the four prompting levels, and the target sound and position are all recorded as you score the session, so the Objective section is a byproduct of doing the therapy rather than a second task afterward.
That capture feeds a template engine, not a blank page. The Objective line is populated from session data through a merge-field system — 20 distinct placeholders such as {studentName}, {soundSymbol}, {position}, {accuracy}, {correctWords}/{totalWords}, and {promptingLevelName} — so the numbers you scored flow into the note’s sentences instead of being retyped. The point isn’t the placeholders; it’s that the most error-prone, time-consuming part of the note is the part that’s automated.
A Copy-Ready Cue-Level Vocabulary Table
Cue level is what separates a defensible Objective section from a vague one, but only if you use precise vocabulary. The clinical cueing hierarchy runs Maximal → Moderate → Minimal → Independent, and it crosses with cue types: verbal/auditory, visual (a gesture or pointing to the articulators), tactile, and orthographic. The table below is the bookmarkable reference — it gives you both the standard clinical language and the exact phrasing to paste, and it maps each level onto what Sound Safari records:
| Cue level | App prompting level | Cue types in play | Ready-to-paste phrasing |
|---|---|---|---|
| Maximal | Maximum (Picture + Word + Model) | Verbal model + visual + tactile | ”given maximal cues (verbal model + visual gesture + tactile placement cue)“ |
| Moderate | Moderate (Picture + Word) | Verbal + visual | ”given moderate cues (verbal model + picture support)“ |
| Minimal | Minimal (Word only) | Single verbal prompt | ”with minimal cues (single verbal prompt)“ |
| Independent | Independent (Picture only / no prompts) | None | ”independently, without clinician cues” |
The clinical principle behind the table is that support is faded systematically over time toward independence. That’s why the cue level in the Objective section is load-bearing: a later Assessment that says “ready to fade prompts” is only defensible if your earlier notes show the cue level dropping in a deliberate sequence. Without documented cue levels, “ready to fade” is an opinion; with them, it’s a trend.
Because the table doubles as a teaching reference, it’s also useful for clinical fellows and new clinicians who are still building the muscle memory for precise cueing language — hand it over rather than re-explaining it.
The Assessment Section: Interpreting the Data (Not Restating It)
If there is one documentation mistake named more than any other, it’s restating the Objective data as the Assessment. “Client scored 80%” is not an assessment — it’s a number you already wrote one section ago. The Assessment must interpret. The job of this section is to answer “what do the numbers mean?”, and that always involves comparison, judgment, or a clinical inference the raw number doesn’t carry on its own.
Data restated (wrong): “Client produced /r/ at 80% accuracy with moderate cues.”
Data interpreted (right): “Accuracy improved 20 points across three sessions, from a baseline of 60%, indicating readiness to advance to the phrase level and begin fading to minimal cues.”
The second version compares the session to something. That’s the move — and it’s also where the data spine pays off, because an interpretation is only as good as the baseline it’s compared against.
This is where Sound Safari makes the Assessment evidence-anchored rather than impressionistic. The note compares the session’s accuracy to a clinically meaningful baseline using a three-tier lookup, in priority order:
- The active IEP goal baseline for that sound and position, if one exists.
- Otherwise, the most recent matching probe.
- Otherwise, the first prior scored session, labeled “initial performance.”
The distinction that matters clinically: this is a true baseline — a fixed reference point — not a rolling average of recent treatment sessions. Comparing today’s 80% to a true baseline of 60% is a defensible progress statement; comparing it to a moving average that’s already absorbed the improvement understates the gain. The merge-field engine builds the comparison sentence automatically through the {progressStatement} and {comparisonStatement} placeholders, so the resolved baseline becomes a written sentence without you doing the arithmetic.
For an age-anchored “ready to advance” or “appropriate to target” claim, tie the Assessment to developmental norms. Sound Safari stores 90%-mastery ages for 24 sounds, sourced from McLeod & Crowe (2018), the current cross-linguistic gold standard, in the years;months format (so 7;0 means 7 years, 0 months — not 7.0 years):
| Sound | 90% mastery age |
|---|---|
| /s/ | 5;0 |
| /r/ | 6;0 |
| /th/ (voiceless) | 7;0 |
So an Assessment for a 6-year-old with a lateral /s/ can defensibly state the sound is past its 90% mastery age and appropriate to target; a /th/ Assessment can note the late 7;0 norm before claiming the same. The norm turns a judgment into an evidence-anchored one.
One natural inflection worth calling out: the Assessment’s “goal met X of Y consecutive sessions” line is progress-monitoring data for the IEP. The same sentence that interprets today’s session also feeds the goal’s trend. If you’re writing or auditing the goals these notes report against, our IEP goals for articulation guide covers goal-writing structure and probe conventions in depth — the SOAP Assessment and the IEP probe are two views of the same data.
The Plan Section: Next Steps Keyed to Performance
The Plan answers “what next?” and should contain: the target for the next session, any cue-level adjustment, position or hierarchy-level advancement, a home-practice assignment, and any goal or discharge-criteria notes. The Plan is where the session’s data turns into a decision.
Sound Safari auto-generates recommended next steps keyed to both the session’s accuracy and its prompting level. The accuracy thresholds drive the logic:
| Accuracy band | Auto-generated Plan direction |
|---|---|
| ≥ 90% | Reduce prompting / advance position / begin generalizing |
| ≥ 80% | Solidify at the current level; introduce varied contexts; begin caregiver home practice |
| ≥ 60% | Maintain cue level; add home practice |
| < 60% | Increase support; drop a level |
It also surfaces discharge-criteria and phonological-awareness flags when the data warrants them. Here’s the logic made concrete across three bands:
90%+: “Fade to minimal cues and advance to the phrase level next session; introduce structured-sentence targets.”
60–79%: “Maintain moderate cues at the word level; assign 10 initial-position home-practice words; re-probe in two sessions.”
Under 60%: “Increase to maximal cues and drop to the syllable level; reduce target-word set to high-frequency CV combinations.”
As with the other sections, the Plan populates from the same session data via merge fields — {recommendedNextSteps} and {homeworkSection} — which closes the loop from practice to documentation: the numbers you scored become the recommendation you’d have written anyway.
The home-practice piece deserves a note. Next-session home practice can be assigned to the student and its results flow back into the data, so the Plan’s “assign home practice” line isn’t a dead end — the parent practice feature captures what happens between sessions and returns it. (Frame this for yourself, not the family: the parent-facing surface never uses clinical documentation language.) And when the Plan advances a specific sound, it’s worth linking your own thinking back to the technique — for example, a Plan that moves /r/ toward conversation pairs naturally with our /r/ sound therapy guide.
Four Complete Copy-Ready Articulation SOAP Notes
Most competitor articles give you one-line Objective fragments. Below are four complete four-section notes spanning the articulation hierarchy — word level through conversation, plus a cluster note — each using student initials (never full names) and each demonstrating the interpret-don’t-restate Assessment rule and the cue-level vocabulary from earlier sections.
Note 1 — Initial /r/ at the word level (moderate cues). A common mid-treatment articulation session.
S: Caregiver reports T.M. practiced /r/ word cards twice this week. Student arrived on-task and engaged throughout (engagement: Good). O: T.M. produced /r/ in the initial position of single words with 75% accuracy (15/20) given moderate cues (verbal model + picture support). A: Accuracy improved 15 points over the IEP baseline of 60%, indicating steady progress within the word level; not yet ready to fade cues or advance position. P: Maintain moderate cues at the word level; expand target-word set to include two-syllable initial-/r/ words; assign 10 home-practice words; re-probe next session.
Note 2 — Final /s/ at the sentence level (minimal cues). Near-mastery; for the lisp-shaping background, see the /s/ sound therapy guide.
S: Student reports practicing “all week” and self-corrected several productions spontaneously. Engagement: Excellent. O: S.R. produced final /s/ in structured sentences with 90% accuracy (18/20) given minimal cues (single verbal prompt), with no lateral or interdental distortion observed. A: Accuracy exceeds the 80% mastery criterion for a second consecutive session and approaches independence at the sentence level, indicating readiness to generalize to conversational contexts. P: Advance to conversational probes next session; reduce to independent productions; assign home practice in connected speech (short retells); begin tracking toward the conversation-level goal.
Note 3 — Voiceless /th/ at the conversation level (independent). A generalization probe; the Assessment addresses the late norm.
S: Classroom teacher reports /th/ errors are “much less noticeable” in group discussion. Engagement: Good. O: During a 3-minute conversational sample, A.K. produced voiceless /θ/ correctly in all word positions with 85% accuracy independently (no clinician cues). A: Performance is well above the 80% conversational criterion and consistent with mastery; given /th/’s late 90%-mastery age of 7;0 per McLeod & Crowe (2018), this level of generalized accuracy supports movement toward discharge for this target. P: Collect one additional generalization probe in the classroom setting; if accuracy holds ≥ 80%, begin discharge-criteria documentation for /θ/; reduce session frequency for this goal to maintenance.
Note 4 — /s/-blend cluster reduction at the word level (maximal cues). Framed as a pattern, not a single sound; see the phonological processes guide.
S: Caregiver reports inconsistent home practice (2 of 5 days) due to a busy week. Student fatigued near session end (engagement: Fair). O: J.L. produced /s/-blends (/sp/, /st/, /sk/) in the initial position of single words with 55% accuracy (11/20) given maximal cues (verbal model + visual gesture + tactile placement cue), most errors being cluster reduction to the second element. A: Accuracy remains below the 60% threshold and reflects a persistent cluster-reduction pattern rather than a single-sound distortion, indicating the target is appropriately framed as phonological rather than purely articulatory; not ready to fade support. P: Increase support — maintain maximal cues and reduce the target-word set to high-frequency /sp/ and /st/ words; add a slowed-model home-practice routine; re-probe in two sessions.
Each note is internally consistent with the rules from earlier: the cue vocabulary is precise, and every Assessment interprets against a baseline or a norm rather than re-stating the percentage.
SOAP vs DAP: Which Format for Articulation Caseloads?
Both SOAP and DAP notes end with an Assessment and a Plan. The difference is the front half: a DAP note merges Subjective and Objective into a single Data section. That makes DAP faster to write but less granular — you lose the explicit separation between what was reported and what was measured.
For school-based and articulation SLPs specifically — the audience the generic mental-health comparisons rarely address — the practical guidance is this:
- DAP is often fine for routine, high-volume articulation sessions. When the “subjective” content is just an engagement rating and the data is a clean accuracy-with-cue-level line, collapsing them into one Data section costs you nothing and saves a few keystrokes per note across a 50-student caseload.
- SOAP’s Subjective/Objective split earns its keep for complex cases, team and IEP contexts, and insurance or medical-necessity justification. When a payer or an IEP team needs to see that the report and the measured data agree — or when the caregiver report is itself clinically meaningful — the clean separation is worth the extra structure.
This is a format choice, not a compliance requirement — which leads directly to the question vendor blogs almost never answer honestly.
Are SOAP Notes Required? What ASHA and Medicare Actually Say
Here’s the part that out-credentials most documentation-vendor blogs: ASHA does not require the SOAP format. Verbatim, from ASHA’s documentation-in-schools FAQs:
“The SOAP note format (Subjective/Objective/Assessment/Plan) is not always used in school settings, but is a good method to ensure your notes include all appropriate information.”
The actual requirement is simpler and more demanding at once: document the service provided and the student’s performance, such that another SLP could read your note and know what to do next. SOAP is a reliable way to hit that bar — it’s a checklist that’s hard to leave a hole in — but it is not the bar itself.
Medicare is the same story with different elements. Per ASHA’s Medicare documentation guidance, the outpatient-therapy record must include an evaluation, a plan of care, daily treatment notes, progress report(s), and a discharge note. The progress report is what justifies the medical necessity of ongoing treatment, and a progress note doesn’t have to be a separate document from a daily treatment note as long as it contains the required elements. SOAP is, again, a vehicle for carrying those elements — not a mandate.
Two compliance guardrails belong here, stated plainly. Sound Safari is a clinical tool, not a medical device: it does not provide diagnoses or treatment recommendations, and it does not replace clinical judgment. And it is not HIPAA compliant — no Business Associate Agreement is available — which is exactly why the sample notes above use student initials rather than full names. FERPA compliance is the user’s responsibility. None of that changes whether your notes are good; it changes how you handle identifiers inside them.
From Practice to Documentation: Closing the Loop
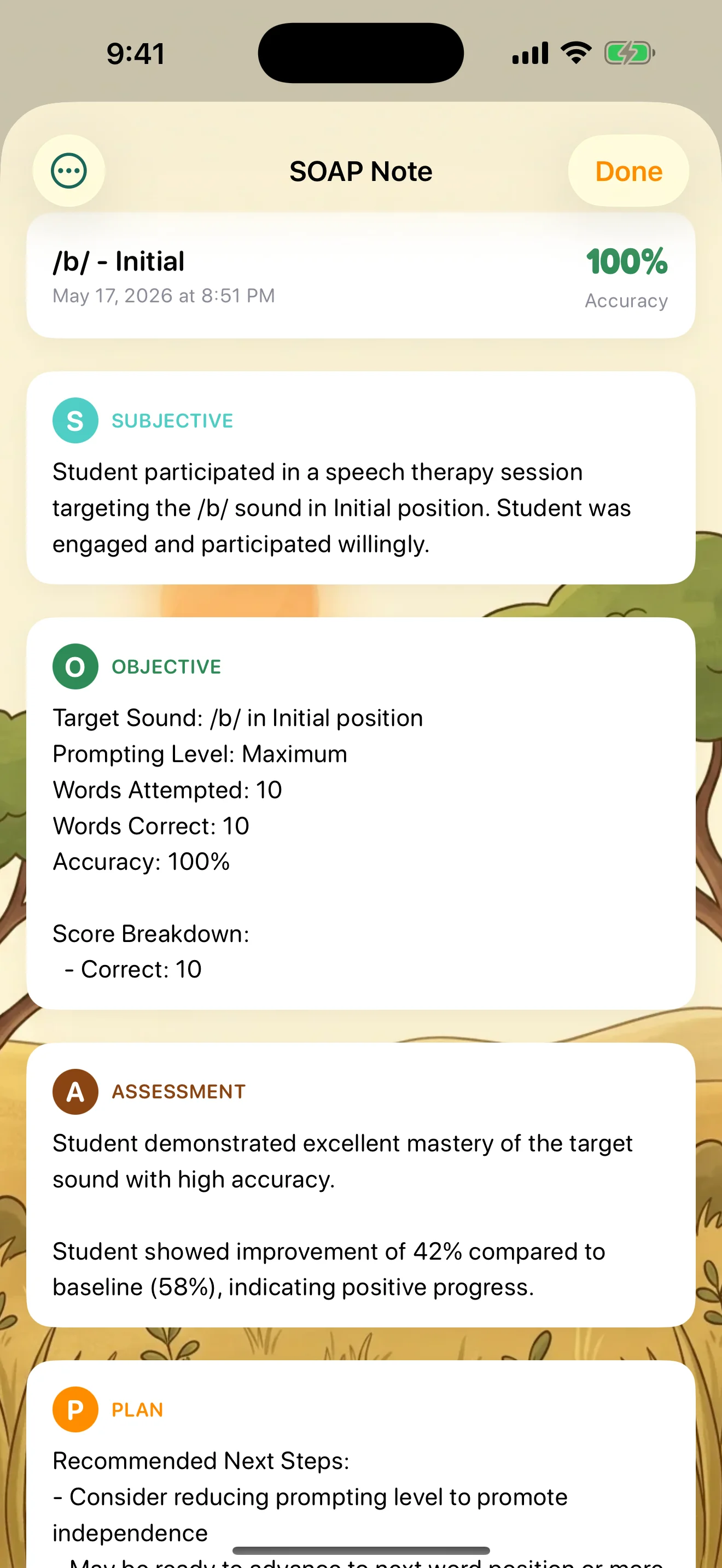
Pull the thesis and the mechanics together. Sound Safari ships two built-in SOAP templates: Standard SOAP — a full note with engagement, scores, and progress and recommendations — and Brief SOAP — a concise note with the key metrics and accuracy. You can duplicate either one and customize it. The note auto-generates from session data through the 20-merge-field engine, so nothing starts from a blank page.
On trust: notes and templates live in the same iCloud-synced store as the rest of the app’s clinical data. Your clinical and student data stays on your device and in your iCloud — it never touches our servers. (No third party ever receives your clinical or student data; account and subscription data are handled separately, with no ads, no behavioral tracking, and no data brokers.)
Disclosed honestly: SOAP note generation is a Pro-tier feature. The in-app lock card reads “Auto-generate clinical notes with Standard or Brief templates,” and it sits behind the subscription.
So the loop, restated end to end: you score during practice (three-point scale plus prompting level) → the Objective section populates from that data → the Assessment compares it to the three-tier baseline → the Plan keys the next steps to the accuracy band → optional home practice is assigned → that data returns. Documentation becomes a byproduct of the session instead of a task after it. That’s the whole pitch, and it’s why Sound Safari is the only articulation app with auto-generated SOAP notes — see /professionals for the clinical feature set or /pricing for plans.
Frequently Asked Questions
What is a SOAP note in speech therapy?
A SOAP note is a structured clinical note with four sections — Subjective, Objective, Assessment, and Plan. In speech therapy it documents what the client or caregiver reported and how the session felt (Subjective), the measurable session data such as accuracy percentage and cue level (Objective), your clinical interpretation of that data (Assessment), and the next steps (Plan). The format comes from Dr. Lawrence Weed’s problem-oriented medical record and is widely used because it ensures a note contains everything another clinician would need to continue care.
What goes in each section of a speech therapy SOAP note?
Subjective: caregiver/teacher report, the student’s self-report, and observed engagement and affect. Objective: the measurable data — target sound, word position, level of the articulation hierarchy, accuracy percentage (correct/total), and cue or prompting level. Assessment: your interpretation of that data, such as comparing it to a baseline and stating readiness to advance. Plan: the target for next session, any cue-level or level adjustment, home practice, and goal or discharge notes. Each section answers one question: how did it feel, what are the numbers, what do they mean, and what next.
How do you write the Objective section of an articulation SOAP note?
Report five measurable elements: target sound, word position, level of the articulation hierarchy, accuracy percentage as a fraction (correct/total), and cue level. A defensible line reads: “Client produced /r/ in the initial position of single words with 80% accuracy (16/20) given moderate cues.” Avoid vague narrative like “worked on /r/ and did well” — that is not measurable. If accuracy differed by cue level, report each band separately (for example 70% with a gestural cue, 30% without).
What is the most common mistake SLPs make when writing SOAP notes?
Restating the Objective data as the Assessment. “Client scored 80%” is not an assessment — it is a number you already wrote in the Objective section. The Assessment must interpret the data: for example, “accuracy improved 20 points across three sessions, indicating readiness to advance to the phrase level.” Other frequent errors are putting measurable data in the Subjective section, putting subjective impressions in the Objective section, and using vague language like “did well” with no data behind it.
What is the difference between a SOAP note and a DAP note?
Both formats end with an Assessment and a Plan. A DAP note merges Subjective and Objective into a single “Data” section, which makes it faster to write but less granular. A SOAP note keeps the Subjective/Objective split, which matters most for complex cases, team and IEP contexts, and insurance or medical-necessity justification. For routine, high-volume articulation sessions the faster DAP format is often fine; choose SOAP when the cleaner separation of report versus measured data earns its keep.
Are SOAP notes required by ASHA or Medicare?
No. ASHA states the SOAP format “is not always used in school settings, but is a good method to ensure your notes include all appropriate information.” The real requirement is documenting the service provided and the student’s performance so another SLP could read the note and know what to do next. For Medicare outpatient therapy, the record must contain an evaluation, plan of care, daily treatment notes, progress report(s), and a discharge note — SOAP is a vehicle for those elements, not a mandate.
How do you document cue levels (maximal, moderate, minimal, independent) in a SOAP note?
Name both the level on the support hierarchy (maximal, moderate, minimal, independent) and the cue type (verbal/auditory, visual, tactile, or orthographic). For example: “given maximal cues (verbal model plus visual gesture plus tactile placement cue)” or “with minimal cues (single verbal prompt).” The cue level is what makes a later “ready to fade prompts” Assessment defensible, because it shows support was being reduced systematically over time toward independence.
How long should a speech therapy SOAP note be?
Long enough that another clinician could pick up the case and know exactly what happened and what to do next — usually a few sentences per section, not paragraphs. The Objective section carries the most weight and should always include the hard numbers. For routine articulation sessions, a concise note with target sound, accuracy, cue level, a one-sentence interpretation, and a clear next step is sufficient; reserve longer narrative for complex or evaluation visits.
Can an app write speech therapy SOAP notes for you?
It can do most of the work. Sound Safari auto-generates SOAP notes from the data you capture while you score a session — the scoring scale (Correct / Incorrect, plus an optional Approximate score) and four prompting levels populate the Objective section, the Assessment compares the result to a true baseline (the active IEP goal, the most recent matching probe, or the first scored session), and the Plan keys next steps to the accuracy band. It is a clinical tool, not a medical device; it does not provide diagnoses, and it is not HIPAA compliant, so use student initials. SOAP note generation is a Pro-tier feature, and there is a 14-day free trial.
Closing
That’s the full anatomy of a defensible articulation SOAP note: four sections that each answer one question, the interpret-don’t-restate rule that keeps the Assessment honest, a copy-ready cue-level table, four complete worked notes spanning the hierarchy, and the authority context — SOAP versus DAP, and what ASHA and Medicare actually require versus merely recommend.
The throughline holds: a SOAP note should be a byproduct of good practice, not a separate after-hours chore. Get the accuracy, cue level, and target captured during the session, and the four sections nearly fill themselves. Sound Safari is the only articulation app with auto-generated SOAP notes — score during practice and the note is largely written by the time the session ends. Fourteen-day free trial, cancel anytime through Apple.